TBE in Slovenia
Zoran Simonović, Veronika Učakar and Maja Praprotnik
ECDC risk status: endemic
(last edited in May 2025, update for 2024: 79 reported cases)
History and current situation
TBE is endemic in Slovenia, and the incidence rate is one of the highest in the EU. In Slovenia, TBE virus was confirmed for the first time in 1953 with isolation of the virus from a patient’s blood.1 In 1955, the virus was isolated from a tick Ixodes ricinus.2
Notification of TBE cases as well as deaths due to TBE has been mandatory in Slovenia since 1977.3 In the past, case definition for TBE surveillance was not available. It was at the treating physicians’ discretion to establish TBE diagnosis for clinical management purposes and report such cases also for surveillance purposes. In recent years, Slovenia has adopted the EU case definition of TBE for the purposes of epidemiological surveillance.4 Cases with central nervous system involvement and laboratory confirmation or cases with central nervous system involvement and an epidemiological link (exposure to common source – unpasteurized dairy products) are notified. Surveillance data has been collected within the communicable diseases surveillance system by the National Institute of Public Health of Slovenia (NIPH).5
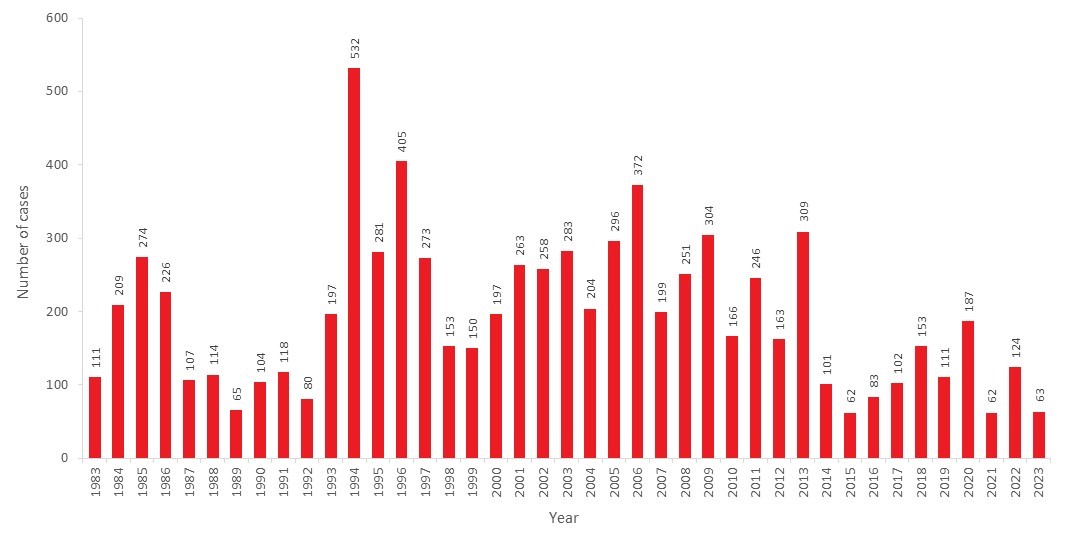
The number of TBE reported cases in Slovenia varies every year. In the period from 1983 to 2023, the number of annually reported TBE cases was between 62 and 532 (incidence rates between 3.0 and 26.6/100,000), which amounts to a mean of 194 cases/year, and a mean annual incidence rate of 9.6/100,000 (Figure 1). In contrast to reports on increasingly higher incidence rates of TBE during the last decade from many EU countries,6 in Slovenia the reported incidence rates during the last decade (2014 – 2023) have decreased compared to the previous two decades (1994 – 2013) (Figure 1). Diverging long-term trends in the occurrence of TBE fluctuates due to multiple factors: virus evolution, climatic factors influencing changes in tick activity and population, number of small forest mammals, as well as human behavior (e.g., changes in leisure activities) play an important role. In addition, changes in surveillance systems, diagnostic methods and vaccination policies can also have an effect on the observed trend.6,7
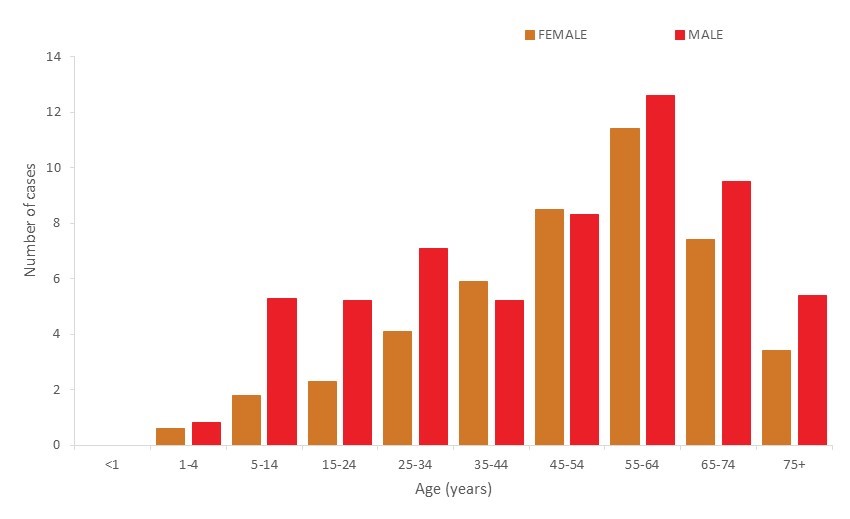
TBE occurs seasonally in Slovenia, usually from May to October, with a peak in June and July, which is linked to tick activity.8 In recent years an increase in the number of the cases in the elderly has been observed.3 Since 2014, TBE incidence rates have been the highest in the 55–64 age group in most years, with males being more frequently affected than females (Figure 2). In men, the 65–74 age group and in women the 45–54 age group followed, with the second highest rates in the period 2014 – 2023. In contrast to the TBE incidence, the disease burden expressed in disability-adjusted life years (DALYs) was higher in children aged 5–14 years than in adults aged 50–74 years.9
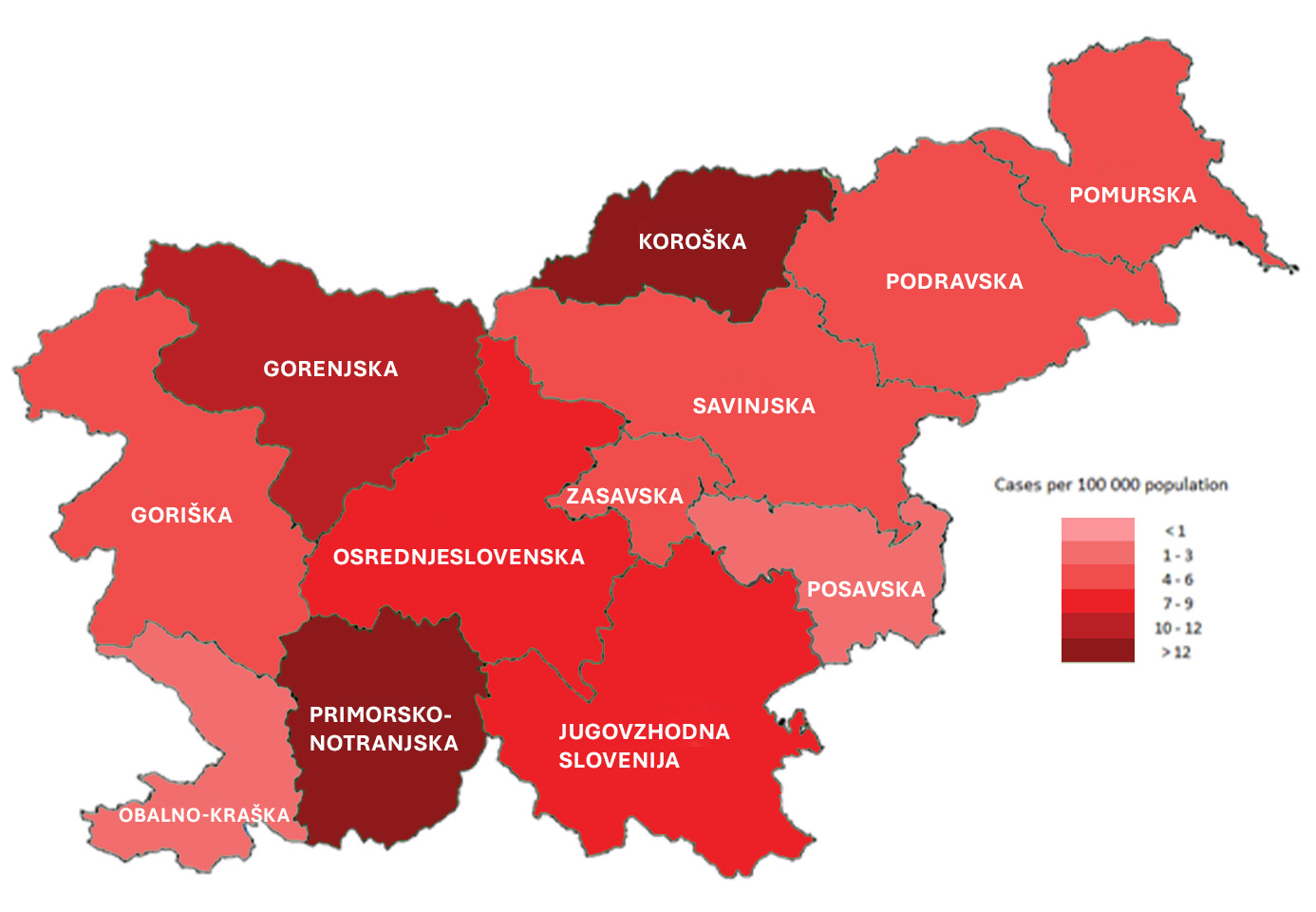
The endemic area for TBE is most of Slovenia, except for the area along the Adriatic Sea. In the past decade (2014 – 2023) cases of TBE were recorded in all Slovenian statistical regions (Figure 3). Although some regions in Slovenia have a higher 10-year average number of TBE cases than others, TBE occurs throughout the country, with the most affected areas in the north and central regions down to the southwestern part of the country, excluding the coastal region.
People who are staying in the endemic areas (temporarily or permanently) have a higher risk for TBE infection. These are mainly people working in forestry, wood and wood-processing industries and construction. The risk is also higher among farmers, if their farmlands are located near forested areas, which present a natural habitat for ticks. There have also been observations of increased TBE incidence among people who visit forests for recreational purpose or forest fruit-picking. An epidemiological study that included 1,564 cases of TBE in Slovenia showed that 82.3% of cases had a tick bite on one or multiple sites on the body. The estimated duration of tick attachment was less than 6 h in 23.5% of TBE cases. Long attachments (more than 24 h) were reported by 10% of the patients. The tick bite occurred while the TBE patients were engaged in leisure time activities (sports or camping, 32.8%), mushroom or berry picking (30.2%), or farming (23.3%). Almost two-thirds of TBE patients reported that they had practiced at least one of the recommended preventive measures, most frequently self-inspection, and least often repellent use.10
Preventive measures against TBE include the use of repellents, appropriate clothing and daily inspection of the skin to remove ticks. The most effective method of preventing TBE is vaccination.11 Mandatory vaccination against TBE was introduced in Slovenia in 1986 for those at risk of occupational exposure, and in 1990 for students at risk of exposure during curricular training, while the rest of the population needed to pay for the vaccination themselves. TBE vaccination coverage in Slovenia remained low: by 2007, the proportion of the general population reporting to ever have been vaccinated against TBE was 12.4%.12 From 2019, Slovenia introduced TBE vaccination for adults and children in the national vaccination program, for children at first after the age of three years then later changed to the age of one year and for adults who reach 49 years of age in the current year. Vaccination for this group is carried out with three doses of vaccine, paid for from the compulsory health insurance. As a general rule, the three-dose basic vaccination is financed. Those who have previously started vaccination on a “self-pay” basis may be vaccinated with the following three doses at the expense of the mandatory health insurance. Vaccination is also available to people who delayed TBE vaccination (children born in 2016 or later and adults who reached 49 years of age in 2019 or later and have not yet received three doses at the expense of the mandatory health insurance).13 In Slovenia the vaccination coverage among children with at least one dose of TBE vaccine enrolled in this program born between 2016 and 2019 ranged from 35.2 – 52.2%. The vaccination coverage among adults with at least one dose of TBE vaccine enrolled in this program born between 1970 and 1973 ranged from 14.7 – 21.1%.14
Overview of TBE in Slovenia
| Table 1: TBE in Slovenia | |
|---|---|
| Viral subtypes isolated | European subtype of TBE virus (TBEV) present in Slovenia. Relatively high genetic variability of Slovenian TBEV with correlation between geographical and phylogenetic clustering was detected.15 |
| Reservoir animals | Rodents; TBEV antibodies were detected in 5.9% of rodent sera. Bank voles had higher rate of infection than mice.16 |
| Infected tick species (%) | In Slovenia the main vector is Ixodes ricinus and the prevalence of TBEV tick infection is 0.47%.17 |
| Dairy product transmission | In previous decades one food-borne outbreak of TBE was reported in Slovenia associated with consumption of raw goat milk (3 cases).18,19 |
| Case definition used by authorities | Slovenia adopted the EU case definition for epidemiological surveillance of TBE.4 |
| Type of reporting | Reporting of TBE cases is mandatory in Slovenia. Cases with central nervous system involvement and laboratory confirmation or cases with central nervous system involvement and epidemiological link (exposure to common source – unpasteurized dairy products) are notified.5 |
| Other TBE-surveillance | Not established |
| Special clinical features | A biphasic course of the illness was reported by 56% of patients. Adults (15 – 60 years old) more often presented with fever, headache, stiff neck and photophobia, whereas seniors (more than 60 years old) more frequently reported fatigue, altered consciousness and decreased muscle strength, these differences indicating a more classic course of TBE in the younger group and a somehow different and more severe acute disease in the older group.20 Direct comparison of clinical and epidemiological characteristics of TBE in children and adults revealed differences in several clinical and laboratory features and corroborates the previous conclusion that TBE in childhood is a milder illness than TBE in adults.21 |
| Licensed vaccines | FSME-IMMUN.22 |
| Vaccination recommendations | TBE vaccination for adults and children included in the Slovenian national vaccination program. For children after the age of one year and for adults who reach 49 years of age in the current year. Vaccination is carried out with three doses of vaccine, paid for by the mandatory health insurance. As a general rule, the three-dose basic vaccination is financed. Those who have previously started vaccination on a “self-pay” basis may be vaccinated with the following three doses at the expense of the mandatory health insurance. As a “catch-up”, vaccination is also available to people who have not yet been TBE vaccinated (children born in 2016 or later and adults who have reached 49 years of age in 2019 or later and have not yet received three doses at the expense of the mandatory health insurance).13 |
| Vaccine uptake | In Slovenia the vaccination coverage among children with at least one dose of TBE vaccine enrolled in national vaccination program born between 2016 and 2019 ranged from 35.2 – 52.2%. The vaccination coverage among adults with at least one dose of TBE vaccine enrolled in this program born between 1970 and 1973 ranged from 14.7 – 21.1%.14 |
| National Reference center for TBE | National Institute of Public Health Trubarjeva cesta 2, 1000 Ljubljana, Slovenia https://nijz.si/ |
Figure 1: TBE case numbers over time, Slovenia, 1983-2023. Update for 2024: 79 reported cases.
| Year | Number of Cases |
|---|---|
| 1983 | 111 |
| 1984 | 209 |
| 1985 | 274 |
| 1986 | 226 |
| 1987 | 107 |
| 1988 | 114 |
| 1989 | 65 |
| 1990 | 104 |
| 1991 | 118 |
| 1992 | 80 |
| 1993 | 197 |
| 1994 | 532 |
| 1995 | 281 |
| 1996 | 405 |
| 1997 | 273 |
| 1998 | 153 |
| 1999 | 150 |
| 2000 | 197 |
| 2001 | 263 |
| 2002 | 258 |
| 2003 | 283 |
| 2004 | 204 |
| 2005 | 296 |
| 2006 | 372 |
| 2007 | 199 |
| 2008 | 251 |
| 2009 | 304 |
| 2010 | 166 |
| 2011 | 246 |
| 2012 | 163 |
| 2013 | 309 |
| 2014 | 101 |
| 2015 | 62 |
| 2016 | 83 |
| 2017 | 102 |
| 2018 | 153 |
| 2019 | 111 |
| 2020 | 187 |
| 2021 | 62 |
| 2022 | 124 |
| 2023 | 63 |
| 2024 | 79 |
Figure 2: Age and gender distribution of TBE cases, Slovenia, 2014-2023
| FEMALE | <1 | 1-4 | 5-14 | 15-24 | 25-34 | 35-44 | 45-54 | 55-64 | 65-74 | 75+ | Total |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 2014 | 0 | 0 | 2 | 2 | 2 | 5 | 7 | 14 | 9 | 2 | 43 |
| 2015 | 0 | 0 | 0 | 3 | 2 | 1 | 4 | 9 | 3 | 4 | 26 |
| 2016 | 0 | 1 | 0 | 6 | 4 | 5 | 4 | 12 | 3 | 4 | 39 |
| 2017 | 0 | 0 | 2 | 1 | 4 | 7 | 8 | 8 | 8 | 1 | 39 |
| 2018 | 0 | 2 | 3 | 3 | 5 | 3 | 14 | 22 | 6 | 8 | 66 |
| 2019 | 0 | 1 | 3 | 1 | 7 | 8 | 9 | 7 | 12 | 4 | 52 |
| 2020 | 0 | 1 | 5 | 3 | 6 | 8 | 15 | 19 | 10 | 5 | 72 |
| 2021 | 0 | 0 | 1 | 0 | 2 | 6 | 7 | 7 | 7 | 0 | 30 |
| 2022 | 0 | 0 | 2 | 1 | 5 | 6 | 13 | 13 | 12 | 5 | 57 |
| 2023 | 0 | 1 | 0 | 3 | 4 | 10 | 4 | 3 | 4 | 1 | 30 |
| Average female | 0 | 0.6 | 1.8 | 2.3 | 4.1 | 5.9 | 8.5 | 11.4 | 7.4 | 3.4 | 45.4 |
| MALE | <1 | 1-4 | 5-14 | 15-24 | 25-34 | 35-44 | 45-54 | 55-64 | 65-74 | 75+ | Total |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 2014 | 0 | 1 | 6 | 11 | 5 | 4 | 8 | 10 | 8 | 5 | 58 |
| 2015 | 0 | 1 | 4 | 4 | 7 | 5 | 4 | 5 | 5 | 1 | 36 |
| 2016 | 0 | 0 | 3 | 4 | 3 | 8 | 5 | 13 | 3 | 5 | 44 |
| 2017 | 0 | 1 | 7 | 4 | 7 | 3 | 13 | 11 | 15 | 2 | 63 |
| 2018 | 0 | 0 | 7 | 6 | 11 | 8 | 16 | 19 | 11 | 9 | 87 |
| 2019 | 0 | 0 | 1 | 5 | 7 | 4 | 13 | 6 | 15 | 8 | 59 |
| 2020 | 0 | 3 | 16 | 10 | 16 | 9 | 11 | 29 | 14 | 7 | 115 |
| 2021 | 0 | 1 | 3 | 1 | 3 | 3 | 4 | 9 | 7 | 1 | 32 |
| 2022 | 0 | 1 | 4 | 6 | 9 | 6 | 4 | 15 | 12 | 10 | 67 |
| 2023 | 0 | 0 | 2 | 1 | 3 | 2 | 5 | 9 | 5 | 6 | 33 |
| Average Male | 0.0 | 0.8 | 5.3 | 5.2 | 7.1 | 5.2 | 8.3 | 12.6 | 9.5 | 5.4 | 59.4 |
Figure 3: Ten-year average incidence of TBE per 100,000 population by statistical region of residence, 2014–2023
Contact
Zoran Simonović
Zoran.simonovic@nijz.si
Authors
Zoran Simonović, Veronika Učakar, Maja Praprotnik
Citation
Simonović Z, Učakar V, Praprotnik M. TBE in Slovenia. Chapter 13. In: Dobler G, Erber W, Bröker M, Chitimia-Dobler L, Schmitt HJ, eds. The TBE Book. 7th ed. Singapore: Global Health Press; 2024. doi:10.33442/26613980_13-30-7
References
- Vesenjak-Zmijanac J, Bedjanič M, Rus S, Kmet J. Virus meningoencephalitis in Slovenia: isolation of the causative agent. Bull WHO. 1955;12:513-20.
- Virus meningo-encephalitis in Slovenia. 4. Isolation of the virus from the ticks Ixodes ricinus. Bull World Health Organ. 1956;15(1-2):275-279.
- Grgič-Vitek M, Klavs I. High burden of tick-borne encephalitis in Slovenia – challenge for vaccination policy. Vaccine. 2011;29:5178-83. doi:10.1016/j.vaccine.2011.05.033
- European Centre for Disease Prevention and Control. EU case definitions. Tick-borne encephalitis. Published July 3, 2018. Accessed March 12, 2024. https://www.ecdc.europa.eu/en/all-topics/eu-case-definitions
- Sočan M, Šubelj M, Grilc E, Frelih T, Grmek Košnik I, Čakš-Jager N. [Definitions of notifiable communicable diseases for the purposes of epidemiological surveillance.]. Nacionalni inštitut za javno zdravje. Published January 15, 2024. Accessed March 12, 2024. https://nijz.si/publikacije/definicije-prijavljivih-nalezljivih-bolezni-za-namene-epidemioloskega-spremljanja/
- Van Heuverswyn J, Hallmaier-Wacker LK., Beauté J, et al. Spatiotemporal spread of tick-borne encephalitis in the EU/EEA, 2012 to 2020. Euro Surveill. 2023;28(11):2200543. doi:10.2807/1560-7917.ES.2023.28.11.2200543
- Pustijanac E, Buršić M, Talapko J, Škrlec I, Meštrović T, Lišnjić D. Tick-Borne Encephalitis Virus: A Comprehensive Review of Transmission, Pathogenesis, Epidemiology, Clinical Manifestations, Diagnosis, and Prevention. Microorganisms. 2023; 11(7):1634. Published 2023 Jun 22. doi:10.3390/microorganisms11071634
- Sočan M, Praprotnik M. [Monitoring of infectious diseases transmitted by arthropods in Slovenia in 2021]. Nacionalni inštitut za javno zdravje. Published September 8, 2023. Accessed March 12, 2024. https://nijz.si/nalezljive-bolezni/spremljanje-nalezljivih-bolezni/spremljanje-nalezljivih-bolezni-ki-jih-prenasajo-clenonozci-v-sloveniji/
- Fafangel M, Cassini A, Colzani E, et al. Estimating the annual burden of tick-borne encephalitis to inform vaccination policy, Slovenia, 2009 to 2013. Euro Surveill. 2017;22:30509. doi:10.2807/1560-7917.ES.2017.22.16.30509
- Blasko-Markic M, Socan M. Tick-borne encephalitis in Slovenia: data from a questionnaire survey. Vector Borne Zoonotic Dis. 2012;12:496-502. doi:10.1089/vbz.2011.0871
- World Health Organization. Vaccines against tick-borne encephalitis: WHO position paper. Wkly Epidemiol Rec. 2011;86(24):241-56.
- Grgic-Vitek M, Klavs I. Low coverage and predictors of vaccination uptake against tick-borne encephalitis in Slovenia. Eur J Public Health. 2012;22(2):182-6. doi:10.1093/eurpub/ckr018
- Nacionalni inštitut za javno zdravje. Klopni meningoencefalitis. Cepljenje – osnovne informacije. Published 2023. Accessed March 12, 2024. https://nijz.si/wp-content/uploads/2023/04/KME-letak-skupni-mar_2023.pdf
- Nacionalni inštitut za javno zdravje. Preliminarno poročilo o precepljenosti otrok in odraslih proti klopnemu meningoencefalitisu v Sloveniji. Published May 1, 2023. Accessed March 12, 2024. https://nijz.si/wp-content/uploads/2023/04/preliminarno_porocilo_KME_10052023.pdf
- Fajs L, Durmiši E, Knap N, Strle F, Avšič-Županc T. Phylogeographic characterization of tick-borne encephalitis virus from patients, rodents and ticks in Slovenia. PloS One. 2012;7(11):e48420. doi:10.1371/journal.pone.0048420
- Knap N, Korva M, Dolinšek V, Sekirnik M, Trilar T, Avšič-Županc T. Patterns of Tick-Borne Encephalitis Virus Infection in Rodents in Slovenia. Vector Borne Zoonotic Dis. 2012;12:236-42. doi:10.1089/vbz.2011.0728
- Durmiši E, Knap N, Saksida A, Trilar T, Duh D, Avšič-Županc T. Prevalence and molecular characterization of tick-borne encephalitis virus in i. ricinus ticks collected in Slovenia. Vector Borne Zoonotic Dis. 2011;11:659-64. doi:10.1089/vbz.2010.0054
- Hudopisk N, Korva M, Janet E, et al. Tick-borne encephalitis associated with consumption of raw goat milk, Slovenia, 2012. Emerg Infect Dis. 2013;19:806-8. doi:10.3201/eid1905.121442
- Elbaz M, Gadoth A, Shepshelovich D, Shasha D, Rudoler N, Paran Y. Systematic Review and Meta-analysis of Foodborne Tick-Borne Encephalitis, Europe, 1980-2021. Emerg Infect Dis. 2022;28(10):1945-1954. doi:10.3201/eid2810.220498
- Logar M, Bogovic P, Cerar D, Avsic-Zupanc T, Strle F. Tick-borne encephalitis in Slovenia from 2000 to 2004: comparison of the course in adult and elderly patients. Wien Klin Wochenschr. 2006;118(21-22):702-707. doi:10.1007/s00508-006-0699-6
- Logar M, Arnez M, Kolbl J, Avsic-Zupanc T, Strle F. Comparison of the epidemiological and clinical features of tick-borne encephalitis in children and adults. Infection. 2000;28(2):74-77. doi:10.1007/s150100050050
- Nacionalni inštitut za javno zdravje. Cepiva proti posameznim boleznim – klopni meningoencefalitis. Published August 27, 2018. Accessed March 13, 2024. https://nijz.si/nalezljive-bolezni/cepljenje/cepiva-proti-posameznim-boleznim-klopni-meningoencefalitis/