TBE in Kazakhstan
Andrey Dmitrovskiy, Zhanna Shapiyeva
ECDC risk status: endemic
(last edited in May 2025, update for 2024: 11 reported cases)
History and current situation
The first isolation of TBEV in Kazakhstan was in the Almaty region by M.P. Chumakov in 1941 (one strain from patient). This is proof that the clinically well-described “spring-summer encephalitis” in the Almaty region was in fact TBE. Later in 1943, 1944 and 1945 the TBEV was isolated from patients by local scientists from the Institute of Epidemiology and Microbiology (IEM), in Alma-Ata by E. I. Demikhovsky from CSF samples and brain tissue.1 TBE clinical manifestations were first described by E.M. Steblov in the Almaty region, and the disease had been named “Almaty encephalitis”. Moreover, Steblov described a chronic variant of TBE as “Kojevnikov’s Epilepsy”.2 In 1954, the TBEV was isolated from Ixodes persulcatus ticks.3 The endemic zone in Eastern Kazakhstan was first characterized by Zhumatov in 1957.4 In 1959, a total of 5 TBEV strains were isolated from 315 Dermacentor reticulatus ticks (in 11 pools – minimal infection rate (MIR) – %14,3) in Zailiysky Alatau and 12 additional strains in Jungarsky Alatau (720 ticks – 12 pools – minimal infection rate (MIR) %13,9).5 In the 1960s the Arbovirus Infections Laboratory of the Institute of Epidemiology, Microbiology and Hygiene (Alma-Ata) under the direction of Zhumatov conducted extensive work to study the natural foci of TBE in Kazakhstan. In particular, for several years, they examined birds for TBEV antibodies in Eastern Kazakhstan using a Hemagglutination Inhibition Assay). In 1961, during the examination of the sera of 46 birds, anti-TBEV antibodies were found in 4 local (non-migratory) species of birds (including jackdaw and starling). In 1962, 2 starlings out of 260 were also found with antibodies to the TBEV, whereas testing of 174 farm animal sera turned out to be negative. At the same time, studies of humans in Eastern Kazakhstan demonstrated seropositivity rates from 1.9% to 19.4%.6 The study of human sera in different endemic regions showed that in mountain foci, where I. persulcatus is common, antibodies were detected in 12.0% of patients whereas in steppe foci it was 4.7%. Of persons between the ages of 11–15 years, antibodies were detected in 0.7%, between 16–25 years in 7.8%, between 26–35 years in 9.9% and over 35 years in 8.3%.
When studying human TBEV infection by different genera of ticks in different endemic territories of Kazakhstan, researchers concluded that in those places with no I. persulcatus ticks patients were infected by Dermacentor reticulatus or Dermacentor marginatus and such infections did not result in any symptoms of TBE.7 All this work resulted in the creation of an epidemiological surveillance network for TBE, including the annual collection and study of ticks for infection rate, tick treatment of farm and domestic animals, as well as in areas where humans are concentrated, and in addition vaccination of the population in endemic areas. Local medical organizations are officially advised to conduct timely identification, recording and reporting of cases, including all individuals affected by tick bites, and this documentation includes diagnostic measures taken, hospitalization, medical examination and treatment of patients with TBE. Clinical supervision for patients who recovered from TBE must be conducted by a neurologist for a two-year period or longer, depending on the patient’s health status. Routine immunization against tick-borne encephalitis must be carried out by medical organizations and must be provided for individuals whose activities are connected with being in a natural focus of TBE.16 The Kazakh Institute of Epidemiology, Microbiology and Hygiene Research defines TBE-endemic areas in the 27 districts and 6 regions of Kazakhstan (Almaty, Eastern Kazakhstan, Akmola, Kostanai, Karaganda and Northern Kazakhstan).13 In 2016, new cases appeared in “old” endemic zones in the Akmola region, in 2020, cases appeared in Northern Kazakhstan region, and in 2022 – in Zhambyl region.17-20 In 2023, the number of confirmed TBE cases had decreased to 24 (32 in 2022), half of cases were registered in Eastern Kazakhstan Region (12). The incidence was still registered in the “new” endemic regions – Akmola – 4 cases and in the Northern Kazakhstan Region – 3 cases. Thus, the data of the former Kazakh Institute of Epidemiology and Microbiology on the wider endemicity of TBE, in addition to the Almaty and East Kazakhstan regions, are confirmed. In this regard, the Ministry of Health of the Republic of Kazakhstan transferred two more regions – Akmola (1 district) and North Kazakhstan (1 district) to the status of endemic regions.21
Overview of TBE in Kazakhstan
| Table 1: TBE in Kazakhstan | |
|---|---|
| Viral subtypes isolated | Siberian subtype, Almaty region12,13 |
| Reservoir animals | Not known |
| Infected tick species (%) | Dermatocentor marginatus, Haemaphysalis punctata |
| Dairy product transmission | Not documented—rare—frequent |
| Case definition used by authorities | Original |
| Completeness of case detection and reporting | The study of human sera in different endemic regions showed that in mountain foci where I. persulcatus is common, antibodies were detected in 12.0% of unvaccinated people whereas in steppe foci it was 4.7%.6 |
| Type of reporting | Mandatory |
| Other TBE-surveillance | Detection in ticks in ELISA and PCR |
| Special clinical features | Monophasic. Risk groups – the local population in endemic regions and those who visit them Clinical manifestation (%) – no information available |
| Licensed vaccines | Tikovak, Baxter AG, Austria, Pfizer Manufacturing Belgium N.V. EnceVir, Microgen, Russia |
| Vaccination recommendations | Local population in endemic regions, and the people working in this area |
| Vaccine uptake | No information available |
| National Reference center for TBE | There is no TBE Reference center in Kazakhstan |
Figure 1: TBE case numbers over time against the background of vaccination. Update for 2024: 11 reported cases.
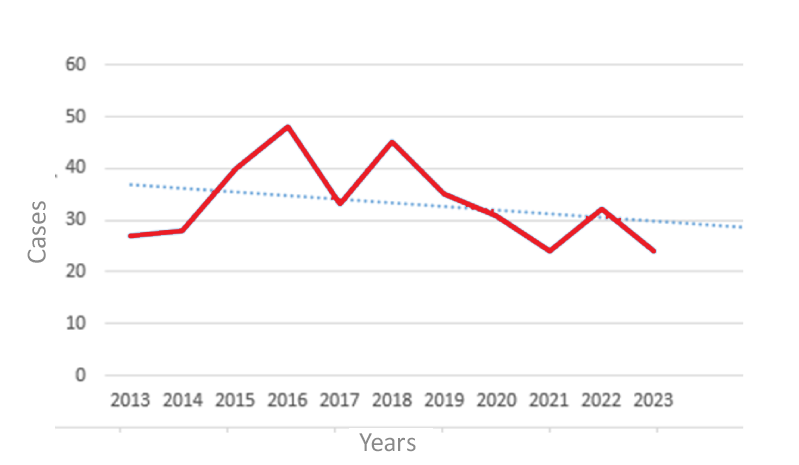
Figure 2: TBE case numbers over time against the background of vaccination

Figure 3: TBEV infection in the regions of Kazakhstan, 1970-2023
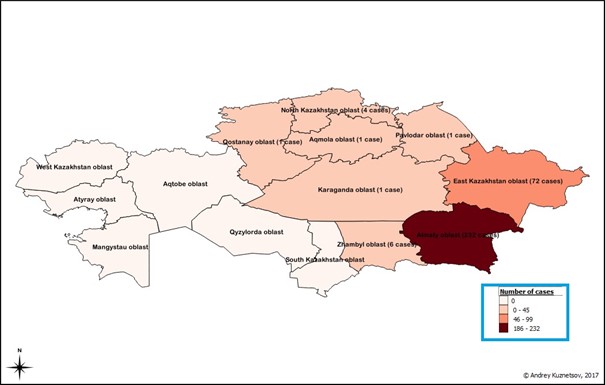
Note: The Kazakhstan Ministry of Health officially considers only Almaty and East Kazakhstan as endemic regions. Data obtained earlier by Prof. Karimov show that additional old TE-foci in fact exist in the country
Maps were created in open source GIS, QGIS ver. 2.8.6 (Wien).
Acknowledgments
TBE surveillance was supported by the Science practical Center for sanitary and epidemiological monitoring and expertise.
Contact
Andrey Dmitrovskiy
am_dmitr@mail.ru
Authors
Andrey Dmitrovskiy and Zhanna Shapiyeva
Citation
Dmitrovskiy A, Shapiyeva Zhanna. TBE in Kazakhstan. Chapter 13. In: Dobler G, Erber W, Bröker M, Chitimia-Dobler L, Schmitt HJ, eds. The TBE Book. 7th ed. Singapore: Global Health Press; 2024. doi:10.33442/26613980_13-17-7