
TBE in Japan
Kentaro Yoshii
E-CDC risk status: affected, possibly endemic
(data as of end 2022)
History and current situation
In Japan the Japanese encephalitis virus (JEV), one of mosquito-borne flaviviruses, has been widely endemic on the main and on the southern islands with more than 1,000 Japanese encephalitis (JE) cases reported annually in the late 1960s.1 In contrast, until 1993, no TBE case had ever been reported and it was considered that there was no endemic focus of TBEV.
In 1993, a case of viral encephalitis in Hokuto city, in the southern part of Hokkaido, was diagnosed as TBE.5 The patient had suffered from fever, headache, and neurological symptoms such as seizures. Hemagglutination inhibition (HI) test against JEV showed significant increase in HI antibodies. However, 2-mercaptoethanol-sensitive HI antibodies were not detected, and it was unlikely that JEV infection occurred in Hokkaido, where JEV was not endemic. Furthermore, blood-sucking vector mosquitoes were not active in the end of autumn in the area. Further serological analysis was conducted against other flaviviruses. IgM-ELISA and neutralization tests revealed very low antibody titer against JEV while high titers of antibodies were detected by neutralization test against TBEV.
Because the patient was a dairy farmer with no history of overseas travel, it was concluded that she had been infected with TBEV by a tick in her living area in Hokkaido. Epizootiological surveys were conducted in Hokkaido, antibodies against TBEV were detected in dogs, horses, racoons, deer and wild rodents in the central to the southern parts of Hokkaido.2-4,7-12 TBEV was isolated from dogs, wild rodents and from Ixodes ovatus ticks, which are the predominant ticks in the area. Sequence and phylogenetic analysis classified the TBEV isolates as Far-Eastern subtype. Besides, antibodies against TBEV were detected in deer and wild rodents in the Tochigi and the Shimane prefectures, and antibodies against the TBEV-serocomplex were also detected in wild boars in wide areas of Japan (the Yamaguchi, Wakayama, Hyogo, Oita, Gifu, Toyama and Chiba prefecture), indicating wide distribution of TBEV all over Japan.3,6,12
Ever since the first confirmed TBE case in 1993, only four additional cases of TBE were reported from Japan, the last one in 2018, although endemic foci of TBEV were detected in various parts of the country, not only in Hokkaido. It is possible that TBE patients are missed in Japan. One major problem is the low awareness for the disease in Japan, even among physicians. Another problem is that commercial tests for diagnostic confirmation of TBEV-infections are not available due to the low awareness and due to the restrictions to handle TBEV in high biosafety level laboratories (BSL 3) only. In Japan, no TBE vaccine is licensed, and it is an urgent medical need to conduct a serological survey among residents in TBEV-endemic areas and to establish preventive measures for residents as well as for travellers to Europe and Russia.
Overview of TBE in Japan
Only five confirmed cases of TBE have been reported from Japan to date. The first patient was a 37-year-old female in 1993,4 and the second patient was a male person in his 40s (2016). The third and fourth patients were male in their 70s (2017). The fifth patient was a female in her 40s (2018). Retrospective survey revealed infection with TBEV in one Lyme disease-suspected patient with meningoencephalitis9 and two asymptomatic cases in Japan Self-Defense Forces members in Hokkaido.10
| Table 1: Virus, vector, transmission of TBE in Japan | |
|---|---|
|
Viral subtypes, distribution |
The Far-Eastern subtype, Hokkaido2,3,5 There is evidence for nationwide – distribution of the TBEV (see text above) |
|
Reservoir animals |
|
|
Infected tick species (%) |
I. ovatus (0.05%–0.33%)8,9 |
|
Dairy product transmission |
Not reported |
| Table 2: TBE reporting and vaccine prevention in Japan | |
|---|---|
|
Mandatory TBE reporting |
Laboratory confirmed cases must be reported by physicians. Case definition: isolation of TBEV or detection of TBEV genomic ribonucleic acid by RT-PCR from blood or cerebrospinal fluid; detection of IgM antibodies against TBEV from blood or cerebrospinal fluid; detection of significant increase in neutralizing antibodies against TBEV in paired serum. |
|
Other TBE surveillance |
No |
|
Special clinical features |
Encephalitis and meningitis with typical neurological symptoms. |
|
Available vaccines |
No |
|
Vaccination recommendations and reimbursement |
No |
|
Vaccine uptake by age group/risk group/general population |
No |
|
Name, address/website of TBE National Reference Center |
No |
Figure 1: TBEV–isolation, TBE cases and animals with TBEV-antibodies in Japan.
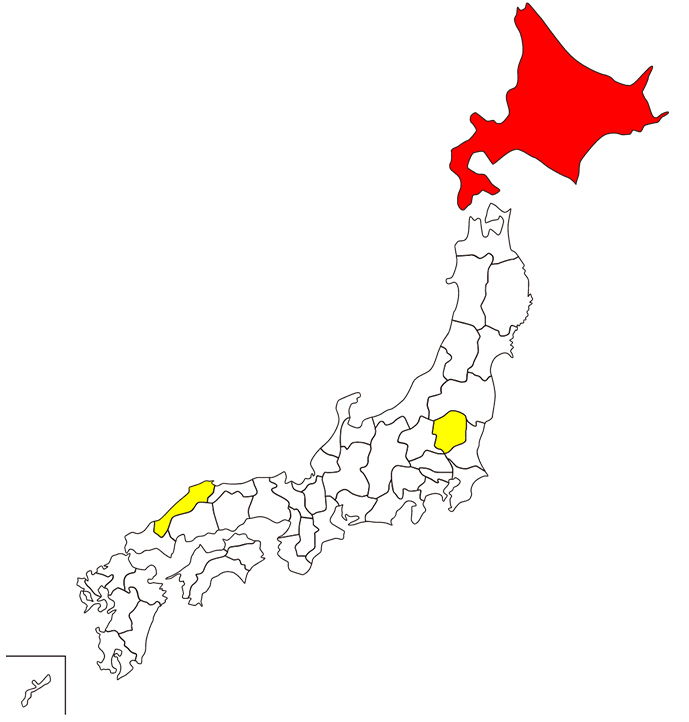
Yellow-colored prefectures: animals were reported.
Contact:
kyoshii@vetmed.hokudai.ac.jp
Citation:
Yoshii K. TBE in Japan. Chapter 12b. In: Dobler G, Erber W, Bröker M, Schmitt HJ, eds. The TBE Book. 6th ed. Singapore: Global Health Press;2023. doi:10.33442/26613980_12b16-6
References
- Arai S, Matsunaga Y, Takasaki T, Tanaka-Taya K, Taniguchi K, Okabe N, et al. Japanese encephalitis: surveillance and elimination effort in Japan from 1982 to 2004. Jpn J Infect Dis. 2008;61(5):333-8.
- Hayasaka D, Suzuki Y, Kariwa H, Ivanov L, Volkov V, Demenev V, et al. Phylogenetic and virulence analysis of tick-borne encephalitis viruses from Japan and far-Eastern Russia. J Gen Virol. 1999;80(Pt 12):3127-35.
- Jamsransuren D, Yoshii K, Kariwa H, Asakawa M, Okuda K, Fujii K, et al. Epidemiological survey of tick-borne encephalitis virus infection in wild animals on Hokkaido and Honshu islands, Japan. Jpn J Vet Res. 2019;67(2):163-72
- Kentaro Y, Yamazaki S, Mottate K, Nagata N, Seto T, Sanada T, et al. Genetic and biological characterization of tick-borne encephalitis virus isolated from wild rodents in southern Hokkaido, Japan in 2008. Vector Borne Zoonotic Dis. 2013;13(6):406-14.
- Morita K, Igarashi A, Sato T, Takezawa T. A suspected case of tick-borne encephalitis in Hokkaido. 1994. Contract No.: 178.
- Shimoda H, Hayasaka D, Yoshii K, Yokoyama M, Suzuki K, Kodera Y, et al. Detection of a novel tick-borne flavivirus and its serological surveillance. Ticks Tick Borne Dis. 2019;10(4):742-8.
- Takashima I, Morita K, Chiba M, Hayasaka D, Sato T, Takezawa C, et al. A case of tick-borne encephalitis in Japan and isolation of the virus. J Clin Microbiol. 1997;35(8):1943-7.
- Takahashi Y, Kobayashi S, Ishizuka M, Hirano M, Muto M, Nishiyama S, et al. Characterization of Tick-borne Encephalitis Virus Isolated From a Tick in Central Hokkaido in 2017. J Gen Virol. 2020;[epub ahead of print]
- Takeda T, Ito T, Chiba M, Takahashi K, Niioka T, Takashima I. Isolation of tick-borne encephalitis virus from I. ovatus (Acari: Ixodidae) in Japan. J Med Entomol. 1998;35(3):227-31.
- Takeda T, Ito T, Osada M, Takahashi K, Takashima I. Isolation of tick-borne encephalitis virus from wild rodents and a seroepizootiologic survey in Hokkaido, Japan. Am J Trop Med Hyg. 1999;60(2):287-91.
- Uchida L, Hayasaka D, Ngwe Tun MM, Morita K, Muramatsu Y, Hagiwara K. Survey of tick-borne zoonotic viruses in wild deer in Hokkaido, Japan. J Vet Med Sci. 2018;80(6):985-8.
- Yoshii K, Mottate K, Omori-Urabe Y, Chiba Y, Seto T, Sanada T, et al. Epizootiological study of tick-borne encephalitis virus infection in Japan. J Vet Med Sci. 2011;73(3):409-12.
- Yoshii K, Sato K, Ishizuka M, Kobayashi S, Kariwa H, Kawabata H. Serologic Evidence of Tick-Borne Encephalitis Virus Infection in a Patient with Suspected Lyme Disease in Japan. Am J Trop Med Hyg. 2018;99(1):180-1.
- Yoshii K, Kojima R, Nishiura H. Unrecognized Subclinical Infection with Tick-borne Encephalitis Virus, Japan. Emerg Infect Dis. 2017;23(10):1753-4.