
TBE in the Czech Republic
Petr Pazdiora
E-CDC risk status: endemic
(data as of end 2022)
History and current situation
The TBE virus (TBEV) was first isolated in the Czech Republic by Czech scientists in 1948-1949 from both a patient and also from Ixodes ricinus ticks.1 However, even before 1948, etiologically unclear summer cases of viral meningoencephalitis had been reported, and likely, at least in part, they are attributable to the TBE virus. These cases were reported mostly from patients in the districts of Beroun (Central Bohemia), Hradec Králové (East Bohemia), Vyškov (South Moravia), and occasionally from the neighborhood of Prague. The official reports of these probable cases of ”tick-borne encephalitis” were registered in the database of the National Institute of Public Health in Prague since 1945.
The first TBEV isolation was accomplished from blood and cerebrospinal fluid of a patient with meningoencephalitis. Other successful isolations were from subjects with a history of a tick bite. The first successful attempt of isolation of the TBE virus from different developmental stages of I. ricinus ticks, collected in forests of the district Beroun, was in 1949. The analysis of an outbreak of meningoencephalitis in Rožňava in south-eastern Slovakia in 1951 from Czech and Slovak specialists ended with the discovery of the alimentary transmission of the TBE virus.
The definition of TBE for reporting changed in the following decades. Following a ministerial decree from 1970, only clinically-manifested, laboratory-confirmed cases of TBE were to be reported to the central surveillance center. The number of case characteristics collected from TBE patients has gradually increased ever since 1982. Since 1993, the national reporting system (EPIDAT) has been computerized. TBE surveillance was established by Regulation No. 275/2010, Annex No. 28.
The Czech Republic is a highly TBE endemic country. Many cases are associated with outdoor activities (camping, living in secondary residences in the countryside, hiking, hunting, fishing, mushrooming), while the incidence of occupational transmission has decreased over the last years (in 2022: 20 cases, i.e., 2.8% among foresters and farmers). Numbers of imported cases from abroad are very low with only 1 case (0.2%) in 2021 and 5 cases (0.7%) in 2022. The geographical distribution of TBE is changing. The gradual spread of TBE into formerly unaffected districts, namely into the border districts of the country at higher altitudes is highlighted. Long-term observations confirm a shift of age-specific incidence rates to older age groups.
The period of the transmission of TBE is changing too. The “TBE-season” with detection of cases is longer than 30–50 years ago and lasts from March to December. These changes of basic epidemiological characteristics may be due to climatic changes, changes of environmental and/or other factors. These factors are affecting the different interactions between TBEV, its vectors and vertebrate hosts too.
Vaccine uptake is very low, the highest rate is reached in the age group of 18–24-year-olds, the lowest among children younger than 4 years; however, there is no central vaccination registry. Data from 8 international telephone surveys in 2009, 2013, 2015, 2018, 2019, 2020, 2021, and 2022 which covered the whole Czech population and defined a “vaccinated person” as someone having received ≥1 dose vaccine uptake, was estimated to be 16, 23, 24, 25, 29, 33, 33 and 38%, respectively. Unpublished data from some Czech regions indicate that vaccine uptake with ≥3 doses is even lower.
Overview of TBE in the Czech Republic
| Table 1: Virus, vector, transmission of TBE in the Czech Republic | |
|---|---|
| Viral subtypes, distribution | European subtype – no other information available |
| Reservoir animals | Apodemus sylvaticus, Apodemus flavicollis, Myodes glareolus, Microtus agrestis, Sciurus vulgaris, Erinaceus roumanicus, Sorex araneus, Talpa europaea15 |
| Indicator animals | Capreolus capreolus, Cervus elaphus, Sus scrofa, Canis lupus, Oeservis ammon, Bos taurus, Capra aegagrus hircus15 |
| Infected tick species (%) | 1970–2022: 156/127,579 (0.122%)16 |
| Dairy product transmission | Rare: 1997–2008: 0.9%11; 1993–2019: 3.4%18; 2022: 0.4%14 Children and adolescents (1993-2019): 6.8%17 |
| Table 2: TBE-reporting and vaccine prevention in the Czech Republic | |
|---|---|
| Mandatory TBE reporting | Each case of TBE is reported by the diagnosing physicians to the respective public health authorities after obtaining positive findings from biological specimens. Only confirmed cases on the basis of clinical and lab criteria are reported.1 |
| Other TBE-surveillance | No information available |
| Special clinical features | Biphasic disease: 1994–1997: 80%15 Children and adolescents (1993–2012): 58%10 Risk groups: no information available |
| % with sequelae: children and adolescents (1993–2012): 3%10 Mortality: case fatality rate (1960–2019): 0.79%17; (1970–2008): 0.55%12; (2018–2022): 0.55%14 Children and adolescents (1960–2019): 0.2%17 |
|
| Available vaccines | FSME-IMMUN (Baxter, Pfizer) since 1990, Encepur (Bavarian Nordic) since 1996. Doses sold: No information available |
| Vaccination recommendations and reimbursement | First recommendation 1990, latest recommendation February 8, 2016. Partial reimbursement from health insurances started in 1993, different strategies of different health insurances in individual years. Total reimbursement from health insurances for people 50 years old and over started in 2022. |
| Vaccine uptake by age group/ risk group/ general population | No valid nationwide information available, results from telephone surveys in 2009, 2013, 2015, 2018, 2019, 2020 and 2021 indicate a vaccine uptake in the general population of 16, 23, 24, 25, 29, 33, 33 and 38%2-9 |
| Name, address/website of TBE National Reference Center | National Reference Laboratory for arboviruses, Public Health Institut Ostrava, Partyzánské nám. 7, 702 00 Ostrava https://zuova.cz/Home/Page/NRL-arboviry16 |
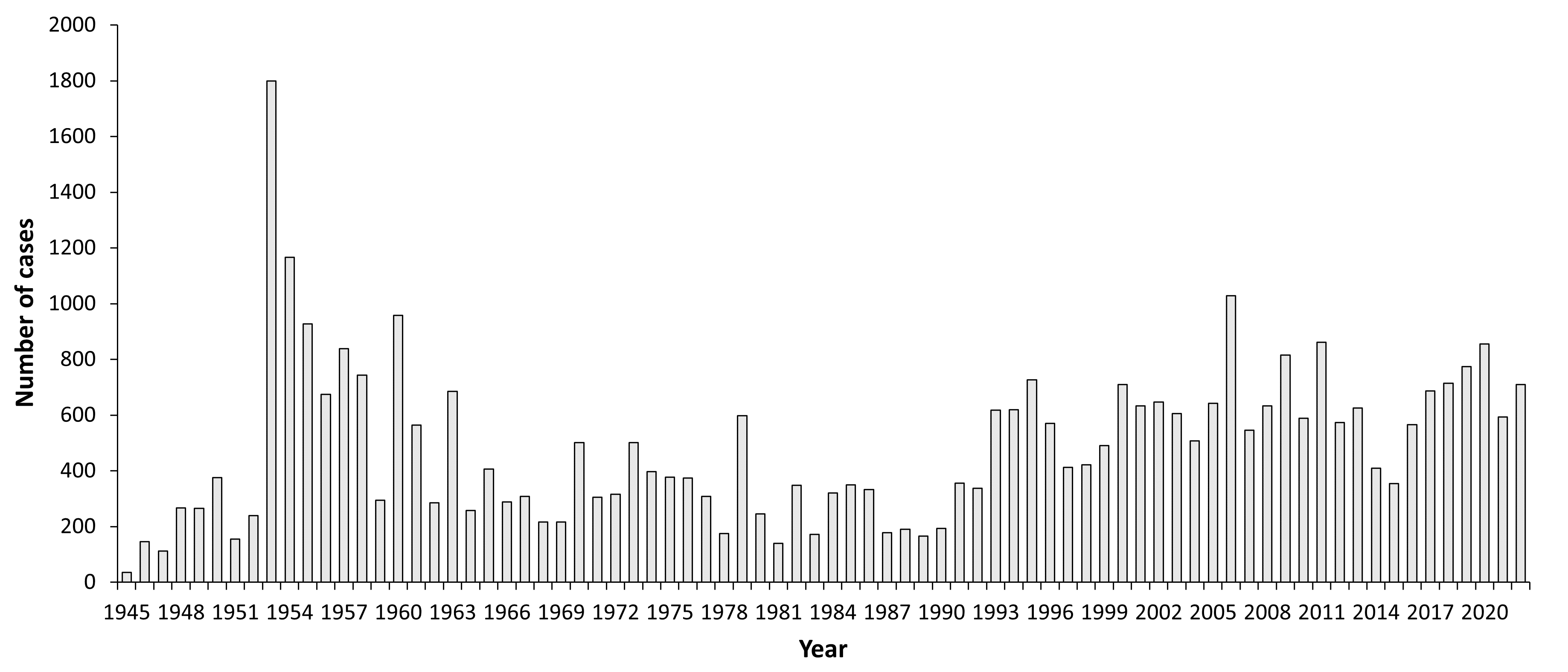
Figure 1: Burden of TBE in the Czech Republic over time14
Click the image above to enlarge
| Year | Number of Cases | Incidence / 105 |
|---|---|---|
| 1945 | 35 | 0.33 |
| 1946 | 146 | 1.53 |
| 1947 | 112 | 1.28 |
| 1948 | 267 | 3 |
| 1949 | 265 | 2.98 |
| 1950 | 375 | 4.2 |
| 1951 | 155 | 1.72 |
| 1952 | 240 | 2.65 |
| 1953 | 1800 | 19.69 |
| 1954 | 1167 | 12.68 |
| 1955 | 927 | 10 |
| 1956 | 675 | 7.23 |
| 1957 | 839 | 8.93 |
| 1958 | 744 | 7.89 |
| 1959 | 294 | 3.11 |
| 1960 | 958 | 9.92 |
| 1961 | 564 | 5.88 |
| 1962 | 285 | 2.96 |
| 1963 | 685 | 7.08 |
| 1964 | 258 | 2.65 |
| 1965 | 407 | 4.16 |
| 1966 | 289 | 2.94 |
| 1967 | 308 | 3.13 |
| 1968 | 216 | 2.19 |
| 1969 | 217 | 2.19 |
| 1970 | 502 | 5.06 |
| 1971 | 305 | 3.1 |
| 1972 | 316 | 3.2 |
| 1973 | 502 | 5.06 |
| 1974 | 397 | 3.97 |
| 1975 | 378 | 3.76 |
| 1976 | 374 | 3.69 |
| 1977 | 309 | 3.0. |
| 1978 | 175 | 1.71 |
| 1979 | 598 | 5.81 |
| 1980 | 246 | 2.38 |
| 1981 | 139 | 1.35 |
| 1982 | 348 | 3.37 |
| 1983 | 172 | 1.63 |
| 1984 | 320 | 3.16 |
| 1985 | 350 | 3.44 |
| 1986 | 333 | 3.22 |
| 1987 | 178 | 4.81 |
| 1988 | 191 | 1.84 |
| 1989 | 166 | 1.6 |
| 1990 | 193 | 1.86 |
| 1991 | 356 | 3.45 |
| 1992 | 337 | 3.28 |
| 1993 | 618 | 6.09 |
| 1994 | 619 | 5.99 |
| 1995 | 727 | 7.19 |
| 1996 | 571 | 5.54 |
| 1997 | 412 | 4.03 |
| 1998 | 422 | 4.1 |
| 1999 | 490 | 4.77 |
| 2000 | 709 | 7 |
| 2001 | 633 | 6.19 |
| 2002 | 647 | 6.34 |
| 2003 | 606 | 5.94 |
| 2004 | 507 | 4.97 |
| 2005 | 642 | 6.28 |
| 2006 | 1028 | 10.02 |
| 2007 | 546 | 5.29 |
| 2008 | 633 | 6.05 |
| 2009 | 816 | 7.78 |
| 2010 | 587 | 5.6 |
| 2011 | 861 | 8.2 |
| 2012 | 573 | 5.45 |
| 2013 | 626 | 5.94 |
| 2014 | 410 | 3.9 |
| 2015 | 355 | 3.4 |
| 2016 | 565 | 5.3 |
| 2017 | 687 | 6.5 |
| 2018 | 715 | 6.7 |
| 2019 | 774 | 7.3 |
| 2020 | 855 | 8 |
| 2021 | 594 | 5.6 |
| 2022 | 710 | 6.8 |
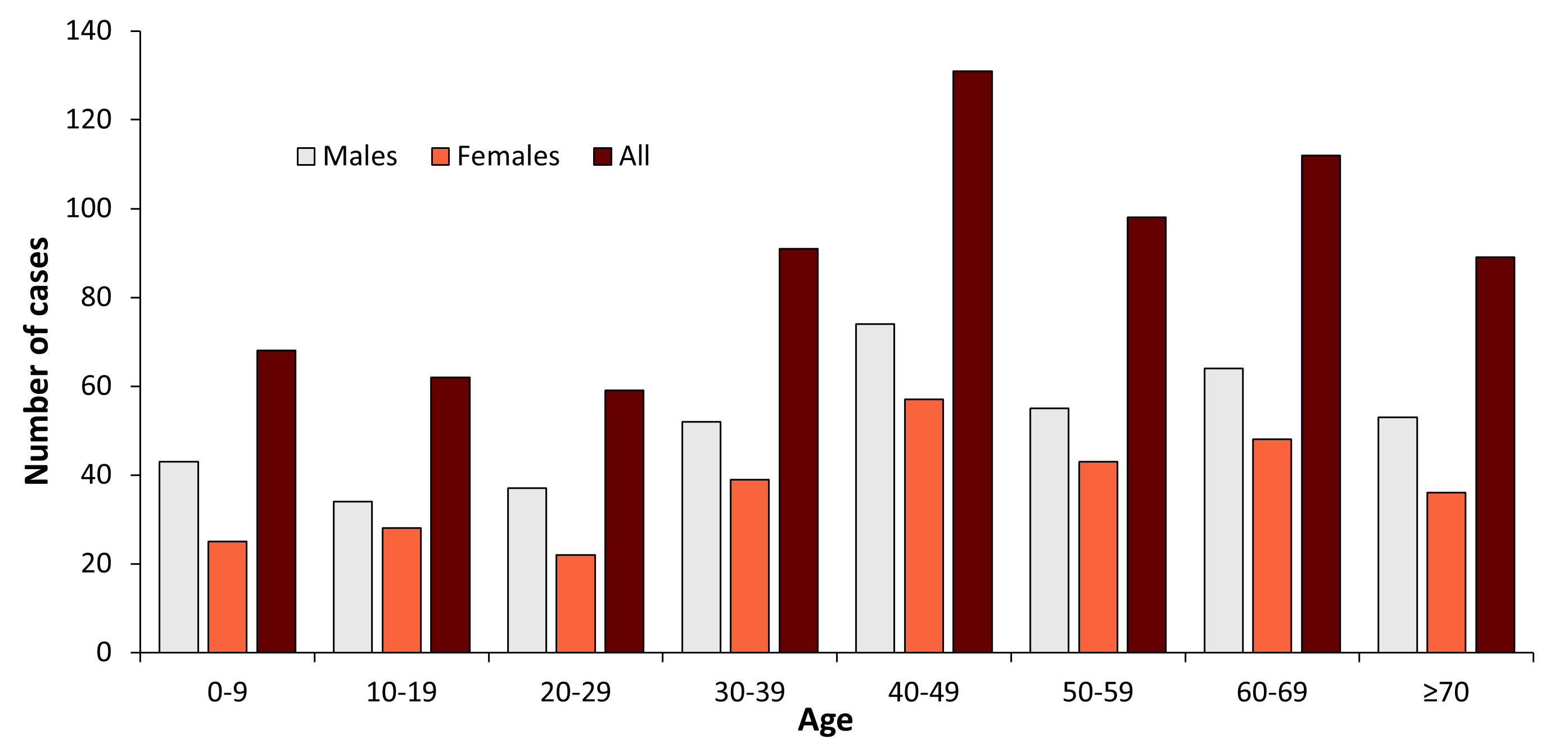
Figure 2: Age and gender distribution of TBE in the Czech Republic (2022)14
Click the image above to enlarge
| Age group (years) | Males | Females | All |
|---|---|---|---|
| 0-9 | 43 | 25 | 68 |
| 10-19 | 34 | 28 | 62 |
| 20-29 | 37 | 22 | 59 |
| 30-39 | 52 | 39 | 91 |
| 40-49 | 74 | 57 | 131 |
| 50-59 | 55 | 43 | 98 |
| 60-69 | 64 | 48 | 112 |
| ≥70 | 53 | 36 | 89 |
| Total | 412 | 298 | 710 |
Figure 3a: Probable TBE cases transmitted in individual regions of the Czech Republic (2022)
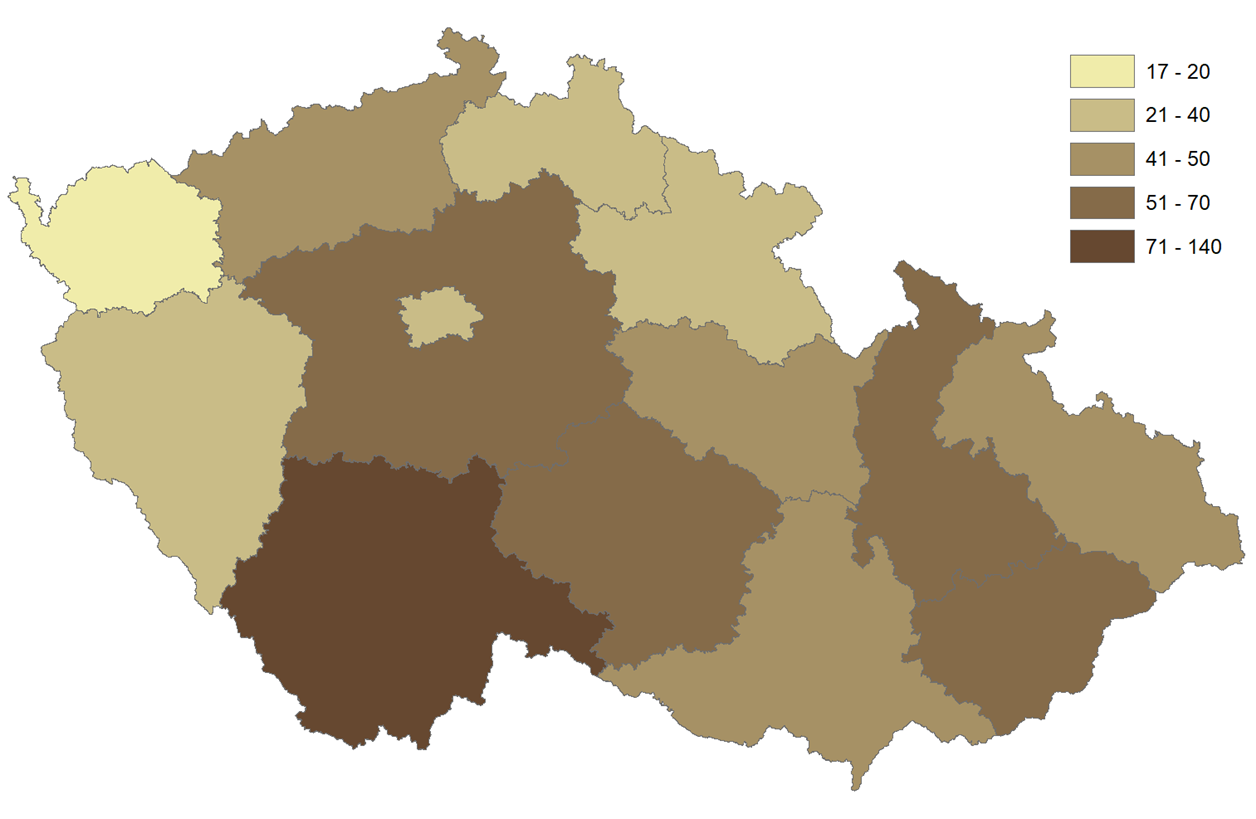
Click the image above to enlarge
Note: Readers may also wish to review the accompanying chapter for Slovakia, given the geographic proximity and national history of these countries. Author’s note: Evidence of reported cases in Czechoslovakia cover the period 1945–1992; cases have been tracked independently in Slovakia since 1993.
Contact:
Citation:
Pazdiora P. TBE in Czech Republic. Chapter 12b. In: Dobler G, Erber W, Bröker M, Schmitt HJ, eds. The TBE Book. 6th ed. Singapore: Global Health Press; 2023. doi:10.33442/26613980_12b8-6
References
- Daniel M, Benes C, Danielova V, Kriz B. Sixty years of research of tick-borne encephalitis–a basis of the current knowledge of the epidemiological situation in Central Europe. Epidemiol Mikrobiol Imunol. 2011;60(4):135-55.
- Fessel – GfK. Tick-borne encephalitis, a study sponsored by Baxter. 2009.
- Fessel – GfK. Tick-borne encephalitis, a study sponsored by Baxter. 2013.
- Fessel – GfK. Tick-borne encephalitis, a study sponsored by Pfizer. 2016.
- Fessel – GfK. Tick-borne encephalitis, a study sponsored by Pfizer. 2018.
- Ipsos: TBE Awareness Coverage and Compliance Research 2019.
- Ipsos: TBE Awareness Coverage and Compliance Research 2020.
- Ipsos: TBE Awareness Coverage and Compliance Research 2021.
- Ipsos: TBE Awareness Coverage and Compliance Research 2022.
- Krbkova L, Stroblova H., Bednarova J. Clinical course and sequalae for tick-borne encephalitis among children in South Moravia (Czech Republic). Eur J Pediatr. 2015174(4):449-58.
- Kriz B, Benes C, Daniel M. Alimentary transmission of tick-borne encephalitis in the Czech Republic (1997-2008). Epidemiol Mikrobiol Imunol. 2009;58(2):98-103.
- Kriz B, Maly M, Benes C, Daniel M. Epidemiology of tick-borne encephalitis in the Czech Republic 1970-2008. Vector Borne Zoonotic Dis. 2012;12(11):994-9.
- Pazdiora P, Struncova V, Svecova M. Tick-borne encephalitis in children and adolescents in the Czech Republic between 1960 and 2007. World J Pediatr. 2012;8(4):363-6.
- Pazdiora P., Gasparek M. The analysis of the register of compulsorily notifiable diseases (EPIDAT 1993-2017; ISIN 2018-2021) – unpublished data
- Růžek D, Danielova V, Daniel M, Chmelik V, Chrdle A, Pazdiora P, et al. Klíšťová encefalitida. 1st ed. Praha; 2015.
- Zelena H. Průkaz viru KE v klíšťatech, Česká republika 1970-2021. 2022; https://zuova.cz/Home/Page/NRL-arboviry.
- Pazdiora P, Prokopova M, Svecova M, Tomaskova H. Tick-borne Encephalitis in Children and Adolescents in the West Bohemian Region (Czech Republic) between 1960 and 2019. The 29th Meeting of the Czech Society for Epidemiology and Microbiology, PED 2020, in Pilsen, the Czech Republic, from 15-17 September, 2020.
- Pazdiora P, Prokopova M, Kudova J, Tomaskova H. Tick-borne Encephalitis in the West Bohemian Region (Czech Republic) between 1960 and 2021. The Meeting of the Czech Society for Epidemiology and Microbiology, Prague, 1st March 2022.